

A 65Yr old female presents to you setting with a 2 week history of intermittent but daily episodes of palpitations described as erratic and irregular, occasional episodes of unprovoked dizziness (once or twice per week) and exertional breathlessness most of the time when climbing up stairs. So what are we looking at here?
One possibility is atrial fibrillation (AF), the most common sustained cardiac arrhythmia in the English population. As a disease with numerous causes it has a significant effect on morbidity, mortality and quality of life. So, we need to try and identify it early and manage patients appropriately and promptly.
There are a few definitions to get our heads around first.
Paroxysmal AF– That is short lived and self limiting but recurrent episodes of AF that last 30 seconds- 7 days (most cases usually terminate <48hrs)
Persistent AF– Episodes that last > 7days. It is worth noting that episodes >7days are unlikely to terminate spontaneously by this point. Or, AF lasting < 7days but that required cardio version to terminate the arrhythmia
Permanent AF– AF that fails to respond to cardio version or that relapses within 24hrs of attempted cardio version.
What is AF?
Rather than the myocardial electrical activity sino atrial node Multiple electrical foci within the atria of the heart cause irregular contraction of the atria myocardium. So frequent are the impulses that the atria are unable to fully contract down and instead fibrillate (think a bag full of live mice wriggling around). The resultant effect is stasis of blood in the atria and incomplete atrial emptying. The problem with this of course is that there is high risk of thrombus formation, and nobody wants rogue clots floating around their blood stream!
Severe cases will result in cardiac ischaemia, haemodynamic instability due to poor cardiac output and that’s before we’ve even considered the thromboembolic complications.
AF has multiple causes, some pathological and some iatrogenic but most commonly associated with hypertension, myocardial infarction and coronary artery disease. Other causes are listed in the box below.

Diagnosis
AF is unlikely in the absence of an irregular pulse, however irregular pulse presence is a poor predictor of AF. Remember that if the AF is intermittent (i.e paroxysmal AF) the patient may not be seeing you in the middle of an episode, which quite frankly is poor planning on their part!
In AF without rate control treatment the ventricular rate is likely to be quite high (160-180bpm), but likely slower than this in older adults.
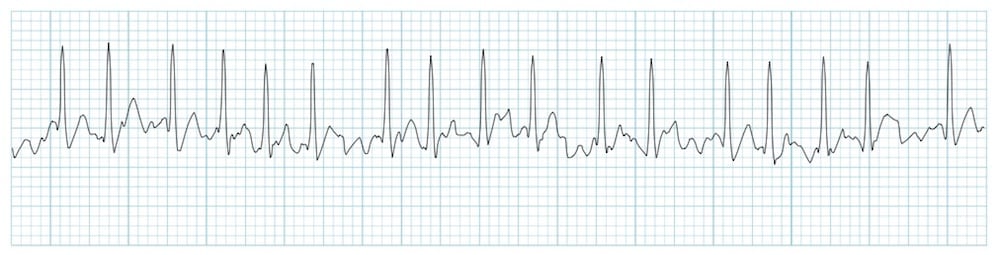
If AF (or indeed any arrhythmia for that matter) is suspected then perform a 12 lead ECG. AF will usually be apparent and characterised by an irregularly irregular ventricular rate, absent P waves and an erratic indiscernible electrical baseline (as seen in the ECG examples below).
If AF is identified on ECG then the diagnosis is clear, but paroxysmal AF (P-AF) poses a little more of a challenge. Suspect P-AF if episodic palpitations or irregular pulse and will likely require a holter monitor to aid diagnosis (if AF not apparent on standard ECG). Episodes of palpitations/ irregular pulse, unprovoked dizziness or syncope should prompt you to consider the possibility of paroxysmal arrhythmia (e.g. AF, VT, sinus arrest etc). The choice of ambulatory monitoring will depend on the frequency of episodes. E.g.a patient having episodes every few days will require a longer period of monitoring than the 24hr standard which will likely miss episodes and be falsely reassuring. If episodes are daily then a 24hr holter would be entirely reasonable. Local availability will of course influence your decisions.
Management
Same day admission for electrical cardio-version if the onset of AF is <48hrs (i.e. < 48hrs symptomatic) AND haemodynamically unstable. In reality most of these cases are likely to be admitted via emergency ambulance if they are significantly unwell.
- Ongoing ischaemic chest pain
- Significantly breathless
- Tachycardia >150bpm and/ or hypotension or evidence of hypo perfusion
- Severe dizziness or syncope
If the patient is stable but AF onset <48hrs, consider management in primary care if deemed appropriate or arrange immediate cardio version via acute medical unit in secondary care. This will depend on patient preferences, risks/ benefits, co-morbidities, service availability etc. If in doubt phone a friend.
The NICE guideline for AF advises us to investigate for an underlying cause and manage accordingly.
- Cardiac causes, such as hypertension, valvular heart disease, heart failure, and ischaemic heart disease — review of the electrocardiogram may identify an old myocardial infarction. Arrange a transthoracic echocardiogram if there is a high risk or suspicion of underlying structural heart disease (such as a heart murmur) or functional heart disease (such as heart failure) that will influence subsequent management (for example choice of antiarrhythmic drug).
- Respiratory causes, such as chest infection or lung cancer — arrange a chest X-ray if lung pathology is suspected and use clinical judgement to determine the need for urgent assessment and referral (see above).
- Systemic causes, such as excessive alcohol intake, hyperthyroidism, electrolyte depletion, infection, or diabetes mellitus — use clinical judgement to determine the need for thyroid function tests, full blood count, and/or blood urea and electrolytes, calcium, magnesium, and glucose measurements.
Treatment is aimed at preventing thromboembolic events and alleviating symptoms. Consider anticoagulation based on the persons risk of embolic stroke stratified using CHA2DS2VASc score but be aware of pitfalls of this tool, and weigh up risk/ benefit in conjunction with their major bleeding risk using the HAS-BLED score.
Anticoagulation will likely be offered to the majority of patients unless they are thought to be low risk based on their CHA2DS2VASc score (i.e. M- <1, F- <2). Warfarin will usually be the first anticoagulant but direct oral anticoagulants (DOAC) (e.g apixaban, dabigatran etc) should be considered where warfarin deemed unsuitable or coagulation is poorly controlled. It is worth mentioning that anticoagulation only reduces rather than eradicates the risk of stroke (64% stroke reduction when using warfarin).
Stroke risk should be regularly reviewed at 65yrs or if at any time the patient develops diabetes, heart failure, peripheral arterial disease, coronary heart disease, stroke or TIA, or systemic thromboembolism.
Rate control treatment is indicated as a first line therapy for the majority of patients with AF. B-blocker or rate limiting Ca+ channel antagonist would be the primary options. Digoxin is only really suitable for those with non P-AF who are sedentary (i.e little or no physical activity). Target resting/ exertional heart rate will depend on the persons age and level of physical activity.
Follow up after 1 wk of commencing rate control treatment to check tolerance and efficacy of treatment. Consider adjusting dose or combination treatment depending on the individual. Refer to cardiology <4wks if rate control fails to eliminate symptoms.
If starting Warfarin check the persons INR daily or every other day until target INR achieved on two consecutive occasions, then twice weekly for 1-2 weeks then weekly thereafter until the target INR is achieved on two occasions. If INR is stable then the monitoring interval can be extended up to 12 wks depending on local arrangements and clinical judgement.
Refer to a cardiologist, people with:
- A pre-excitation syndrome such as Wolff–Parkinson–White syndrome (you really don’t want to have this if you have AF, it makes them really sick! If you don’t believe me, see the horrible looking ECG example 11 and 12 HERE)
- Valvular heart disease associated with AF.
- Suspected heart failure (with or without a previous MI).
Refer to cardiology for consideration for cardio-version, people with AF;
- That has a potentially reversible cause (for example a chest infection).
- Who have heart failure thought to be primarily caused, or worsened, by AF.
Refer to an endocrinologist people with suspected thyroid disease or a pulmonary oncologist if lung cancer is suspected.
Sources
https://cks.nice.org.uk/topics/atrial-fibrillation/[/vc_column_text][/vc_column][/vc_row]


