

This months blog post is a little different to usual, because it is as relevant to parents and carers of children as it is to health professionals seeing children with fever (high temperature). Consequently, the language used here won’t be the usual medical terminology that you’ll see in my other blogs, rather, everyday language so that the information is useful for as many people as possible.
Why?
Fever often causes unnecessary levels of concern for parents and health professionals alike. I know because I see this day in day out! This concern is often based on historic and outdated beliefs about fever and what we should be doing about it. However, as health professionals, we have national clinical guidance from NICE (National Institute for Health and Care Excellence) that has (been trying) to reassure us since at least 2007 (1) that we should be thinking differently about fever in children, and that traditional beliefs have been proven to be incorrect.
A quick Google search will throw up hundreds of sources of ‘information’ about fever, some of it well founded and trust worthy, but some of will be utter crap. A word of advice for people choosing to use ‘Dr Google’ is that you should stick to well researched and trusted sources. The ones below would be my ‘go to’, but there are others I’m sure.
- NHS websites or your GP practice website
- Patient.info
- What0-18.nhs.uk (my personal favourite, it is fantastic source of information for parents AND clinical guidance for health professionals)
- Whenshouldiworry.yolasite.com – Online information booklet.
Yes, right, focus Ben!
In my day to working life in a busy GP practice, Id say that approximately 25-50% of my appointments will be children with a feverish illness and there is nearly always a concern raised by the parent/ carer that specifically relates to the child’s fever rather than the illness itself. Similarly I regularly see cases where children re-attend because of a specific fever- related concern that another health professional has advised them to respond to e.g “if the fever gets worse” or “goes above XX degrees” or “if it doesn’t come down after medicine”.
The concerns might understandably be greater if parents have had previous experience of say febrile convulsions (we will talk more about this later) or a child with a serious infection or sepsis.
The crooks of the matter is that fever gets too much of our focus and attention. If we can start looking at fever in a different way, we should be able to divert our focus to the things that are helpful. For that to happen, I’ll go right back to the fundamentals of what fever is, why it happens and how it affects the child’s inner workings.
What is a fever, and what it is not
Normal body temperature fluctuates between 36- 37.6C but there is no universally agreed definition as to when a fever is a fever. It is widely accepted that 38C or higher is a ‘fever’ and anything between 37.7- 38C is low grade fever, or as I call it, ‘brewing something’.
Fever IS NOT DANGEROUS. It is a NORMAL, deliberate response by the immune system that helps to fight off infection caused most commonly by viruses and bacteria or much less commonly, fungal or parasite infections.
During infection and the fever that can follow (infection doesn’t always cause fever), the hypothalamus (the brain’s inner thermostat) is triggered to increase the body’s temperature in an attempt to make it difficult for the infection to survive or spread. By turning up the ‘thermostat’, the body is tricked into feeling colder than it is, causing a range of behavioural and physiological responses.
- Shivering- generates heat from muscle movement
- Wrapping up warm to conserve heat and reduce heat loss into the environment
- Curling up – children especially can be seen to curl up into a ball to reduce heat loss and keep their body heat close
- Cold peripheries- to raise the core temperature around important vital organs, less important areas like the hands, feet, nose, ears (anything that sticks out on the edges really) receive a reduced flow of blood. This makes the extremities feel cold and often look a bit purple/ blue, but a short time later will feel warm and look normal again. Whereas in serious infection (sepsis) the extremities will become cold and poorly supplied with blood and deteriorate as the infection worsens.
- The Child’s breathing and heart rate will increase. The higher the fever, the higher the heart and breathing rate. Why? Simply because generating a fever uses a lot of energy and oxygen and so the heart and lungs meet this demand by working faster.
The reality is that you will see the child going hot and cold as the body heats up and cools down to maintain the desired temperature.
What does fever tell us about the infection?
Actually, very little! It tells us that the immune system is busy. End of. The numbers are not important. Really! A child with a temperature of 40C isn’t automatically sicker or experiencing a more serious infection than a child with at 38C.
Fever is useful to work out why a child is unwell. Personally, if my children (I have 2 young sons) are grizzly and I don’t know why, checking their temperature can help work out why they’re not happy. It they have a fever, so be it, thermometer goes away for the next few days and out come the drugs… paracetamol and ibuprofen, I’m not Pablo Escobar!
We can work out what type of infection the child has by finding where it is (the source or focus), since we know the kind of ‘bugs’ that will most often cause those infections. We will then have a good idea of how long we can expect them to be unwell for, and what helpful things we could be doing to treat them.
Example 1– A 2 yr old with a fever of 40C being caused by a cold/ cough/ sore throat, who is drinking well and feels a bit better for a short time after having paracetamol is unlikely to have serious illness. In fact they most likely have a viral infection. I can say this even without measuring the temperature because I know the cause and the child looks well(ish) and feels a little better with helpful treatment.
Example 2– A 4 yr old with a cough who looks very breathless, is pale, persistently cold/ mottled hands and feet, is drowsy and looks dehydrated, with a temperature of 37.9C is likely to be very sick and they’re going to be going to hospital pronto! I know this because of how they look and what their body is telling me, and I don’t really care about the temperature because it tells me nothing useful.
Historically, we have been taught a few myths about fever, whether by relatives, friends, TV or social media personalities. Health professionals are just as responsible for (inadvertently) being taught and spreading myths.
- MYTH 1- The higher the fever, the greater the risk of serious illness.
- MYTH 2- Serious illness is more likely if the fever doesn’t come down with medicines like Paracetamol or Ibuprofen.
- MYTH 3- The risk of convulsions/ fits increases the higher the fever.
- MYTH 4- You MUST control the fever as it can cause convulsions/ fits.
- There are others too..
The presence of fever tells us next to nothing about the type or severity of the infection, other than the immune system is actively dealing with it.
Like everything in life, there are a couple of caveats.
- Children less than 3 months of age with temperature 38C or higher are at greater risk of significant infection. Young babies, especially those born early are at greater risk of serious illness anyway, because their immune system is under developed, hence why we vaccinate so much in the first few weeks. This means that their immune system doesn’t behave in the same way as that of older children, and do not usually develop a fever when they an infection. If a child aged less than 3months develops a fever of 38C or higher, there is a good chance that this is being caused by a significant infection, by which I mean an infection that we need to actively treat e.g with antibiotics. Such infections can include urine infection, pneumonia, skin infection, meningitis, infection of both inner ears.
- Children aged 3-6 months with a fever of 39C or higher are at slightly greater risk of important infection but less so than the very young, but we still need to check them over to make sure we aren’t overlooking anything
- After 6 months of age (corrected age if premature) we shouldn’t really pay too much notice to the numbers themselves.
- Children with immune system suppression/ compromise or serious health conditions – e.g on chemotherapy or those with diabetes, significant heart and lung diseases etc, may be at greater risk of serious illness, and fever or other signs of infection should prompt early consultation with GP or other health professional.
Most feverish illnesses will start to improve after 4-5 days, and the fever along with it should start to settle. It is worth seeing a health professional if the child isn’t improving by day 5, or if their fever persists beyond this, so that we can rule out a new important infection ‘piggy backing’ on the original illness. We would also want to exclude a very rare disease called Kawasaki disease that can cause fever and a rash lasting more than 5 days, that only affects around 8 per 100,000 children under 5 yrs old (2) (which is almost as rare as rocking horse poo) and is nothing to do with bright green motorbikes!. It is more common in Japan.
How should we treat fever?
The simple answer, is that we don’t need to. Unless the child is in pain, we don’t need to be giving any medicine, regardless of how hot they are.
Shift the focus to things that might make the child feel more comfortable and ensuring that they drink regularly to avoid dehydration. If they are hot but comfortable, they don’t need medicine. Treating fever without pain simply uses up doses of medicine that could be useful later, say, in the middle of the night when they wake upset and in pain.
Paracetamol and Ibuprofen are fantastically useful medicines to help children feel more comfortable, and should be used regularly if the child is in pain or if the fever is causing them distress (e.g if hallucinating or very unsettled). Give each medicine alternately will usually mean that the effects last longer than if you were to give both together. Using them regularly for a few days is very unlikely to be detrimental (unless your child have liver or kidney problems in which case discuss with your preferred health professional).
Ensure they are drinking regularly, any drink is fine as long as they are peeing regularly, at least twice a day.
If we need to treat the infection that is causing the fever, then we will do this, but it isn’t usually helpful to give antibiotics, since most illnesses in children are caused by viruses or other illnesses that their immune system can deal with in a few days. This is especially true of most coughs, colds, sore throats, ear aches and tummy bugs. I’ll add a link at the bottom for information about specific illnesses and what to look out for so that more important illnesses do not get missed.
Don’t over dress or under dress or try and cool them down since this interferes with the body’s own mechanisms to regulate the fever. Trying to cool them down with fanning, sponging or under dressing is likely to actually make them more uncomfortable and their body work harder to get them hotter. They are likely to start shivering as their skin cools. Remember that their body is trying to warm them up on purpose. Let it do the job it has evolved to do. Think of it like turning your heating on at home and then opening all the doors and windows, your heating system will have to work harder and use more energy to get to the required temperature.
Dressing them or putting them to bed in light clothes/ covers that usual is probably appropriate since it’ll reduce the risk of them overheating when the body wants to cool down. It can’t do this is they are excessively dressed.
Febrile convulsions
A bit of a misnomer, but essentially these are seizures that occur in children during feverish illness, but probably aren’t directly related to the temperature itself. They are fairly common in young children (6m- 3yrs), and around 1 in 20 children will have one. They are less common with increasing age, and rare in children over 5yrs, probably because their immune system is starting to react to illness differently than younger children (3).
Treating the fever, does not reduce the risk of febrile convulsions (1, 4).
Originally thought to be caused by the fever itself, this has been heavily disputed and disproven for at least the last 20yrs but we don’t really know what causes them, but the majority are not caused by serious infection and don’t have any long term complications. That doesn’t stop them being scary as heck and will benefit from being seen by a health professional as soon as possible just to be sure that nothing more serious is going on.
Summary
Fever is a common symptom of infection in children but shouldn’t cause undue concern if the child feels a little better with regular pain reducing medicines and is drinking well.
Since the majority of feverish illnesses in children are caused by viruses, antibiotic or other treatment specifically targeting the infection, are not usually helpful.
Children under 6months old are at greater risk of serious illness and the presence of fever in this group of children should prompt health assessment. Beyond 6 months old, the height of fever is usually not important.
Febrile convulsions are common, can be frightening to experience, but are unlikely to be a serious problem.
Parents know their children better than anyone, if they’re worried, they’re worried for a reason and health professionals should listen and take this seriously!
I hope you’ve enjoyed reading this and found it useful. If you have then please share it and the resources below far and wide. Knowledge is confidence.
Useful resources + references sources.
I love this leaflet, so much so that I give copies to as many parents as I can and it supports everything I’ve discussed here.

Website, children’s health information . Healthier Together: What 0 -18
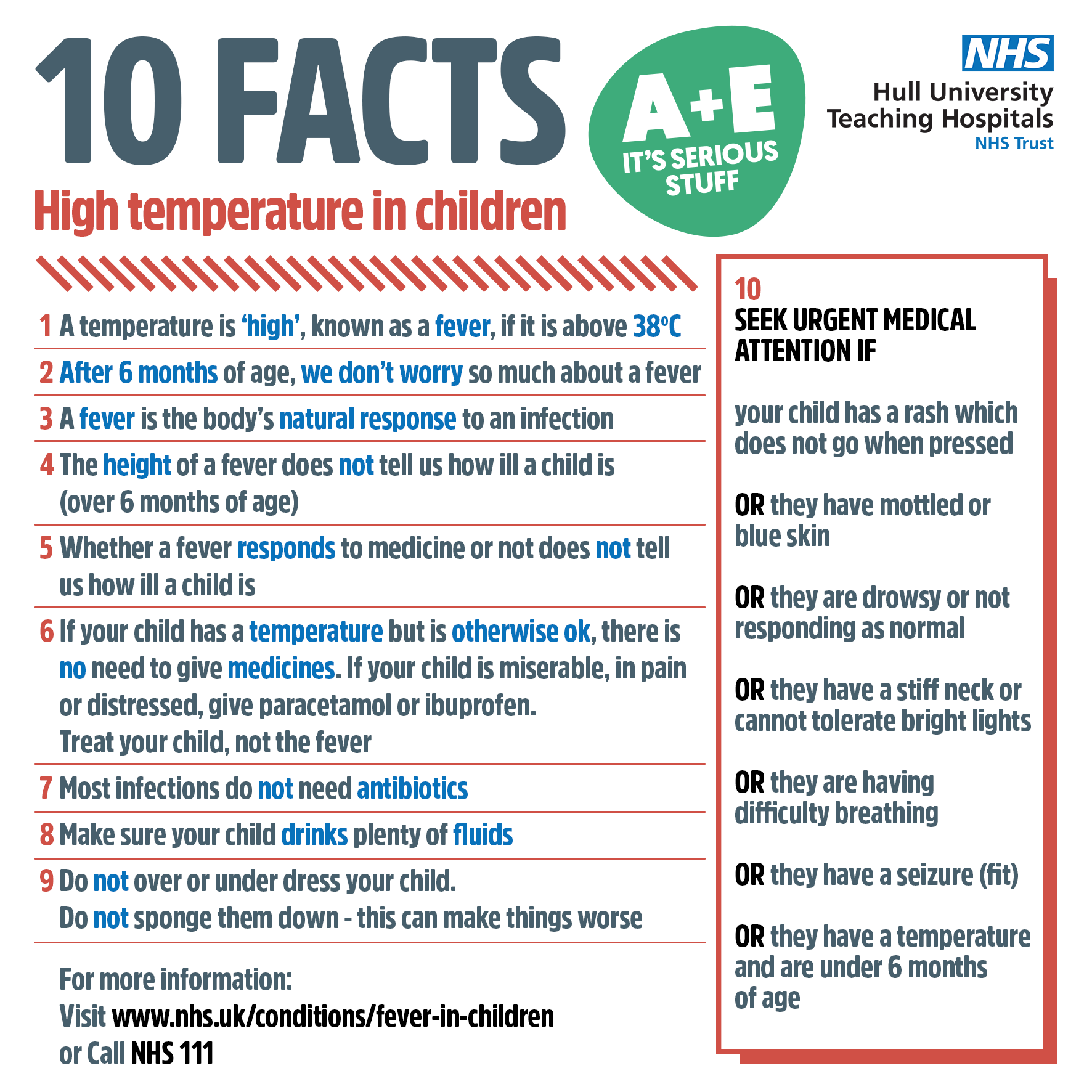
Patient Leaflet. 10 Facts, High Temperature in Children
1- NICE – feverish illness in children under 5
2- Great Ormond Street Children Hospital – Kawasaki disease
3- NHS Inform Scotland febrile convulsions
4- Dr D Capehorn, PULSE Magazine Myth and Facts: Fever in Children



{kind=link}